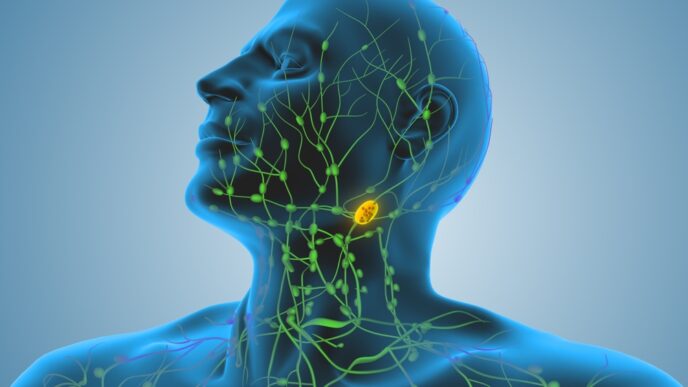
Health An Oncologist Answers: What Exactly Is Lymphoma and How Do We Treat It? byHealthToday Malaysia08/09/2025
Health Malaysian Nurse Named Top 10 Global Finalist in Prestigious International Award. Here’s Her Story byHealthToday Malaysia29/08/2025
Traditional & Complementary Medicine Acupuncture Can Offer Cancer Patients and Survivors Relief from Anxiety and Depression byHealthToday Malaysia06/04/2025
Health Your Burning Questions about Leukemia Answered: Risks & Symptoms byHealthToday Malaysia10/12/2024
Health Your Burning Questions about Leukemia Answered: Diagnosis & Treatment byHealthToday Malaysia10/12/2024
Health An Expert Explains What Many People Tend to Misunderstand about Palliative Care byHealthToday Malaysia17/10/2024
Health Healing Across Genders: The Bald Oncologist Tackles Cultural Norms in Malaysian Cancer Treatment byHealthToday Malaysia20/09/2024
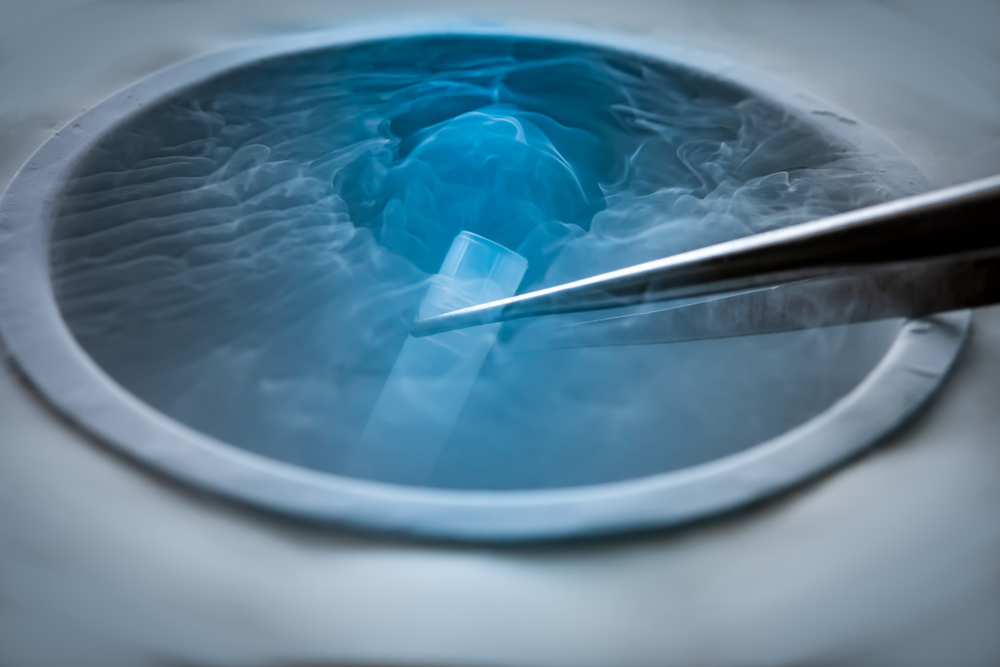
Fertility Ovarian Tissue Cryopreservation Offers Hope for Women with Cancer to Preserve Their Fertility byHealthToday Malaysia07/06/2024
Innovations An Oncologist Spotlights the Newest and Latest in Stereotactic Radiosurgery Technology byHealthToday Malaysia18/01/2024
Sponsored Article A Significant Milestone in Improving the Access of Malaysians to Comprehensive Genomic Profiling byHealthToday Malaysia01/11/2023