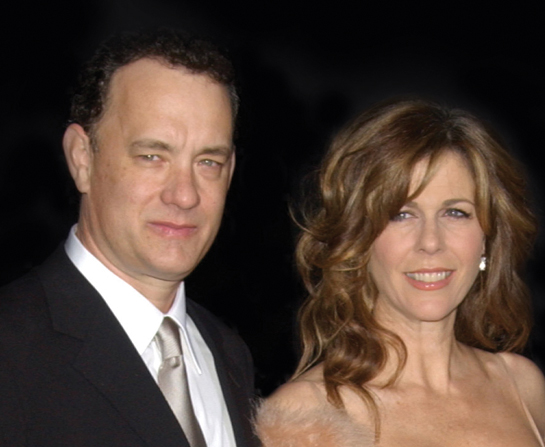
Health Top to Toe Influenza A viral message, more viral than the virus itself byHealthToday Malaysia08/05/2022
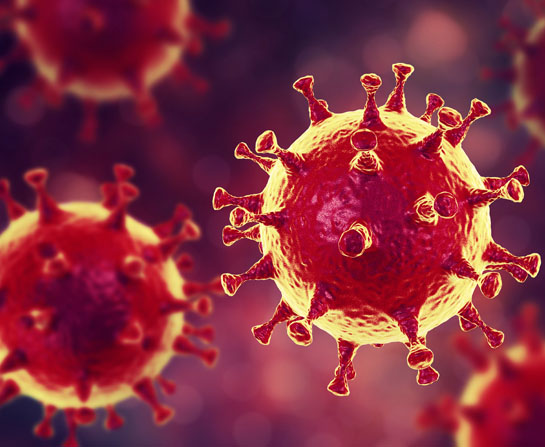
Health Top to Toe CORONAVIRUS 2019-nCoV: A LITTLE COMMON SENSE GOES A LONG WAY byHealthToday Malaysia08/05/2022
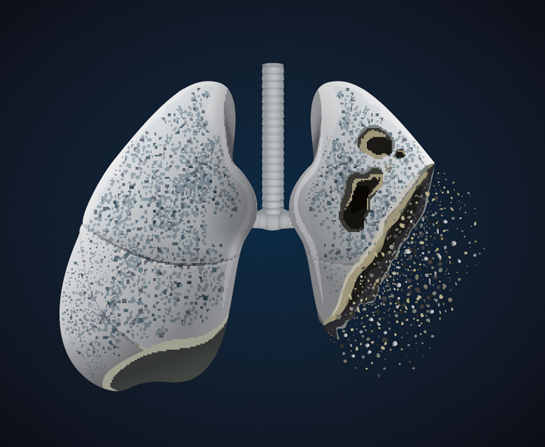
Health Top to Toe Investment Needed for Better Data to Avoid a Potential Surgical Waiting Time Crisis byHealthToday Malaysia08/05/2022